The good news about having a painful shoulder is that most conditions that cause pain around the shoulder can be treated without an operation or surgery. Physiotherapy exercises are the mainstay of treatment and can relieve pain, restore lost movement and strengthen the shoulder. Injections can be used in certain circumstances both for diagnosis and treatment of painful shoulder conditions.

The shoulder is the most mobile joint in the body and is a complex structure made up of the glenohumeral joint, the acromioclavicular joint, the collar bone (clavicle) several ligaments, muscles, tendons and bursae. The main joint between the arm bone (humerus) and wing bone (scapula or glenoid) is a ball and socket joint which allows movement in many directions: forward (elevation), backward (extension), around in a circle (circumduction), and away from the body (Abduction). It can also twist (internal and external rotation). Unlike the hip joint which is large and deep (and relies on bone shape to keep it in joint), the shoulder relies on the muscles and ligaments to help keep it stable and secure in its socket.
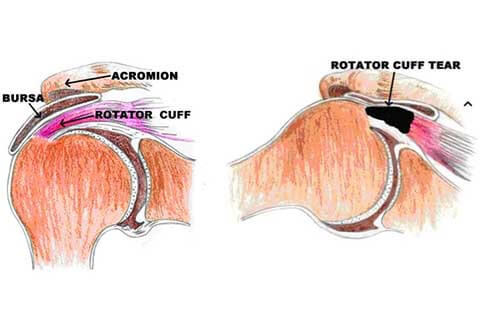
Rotator Cuff
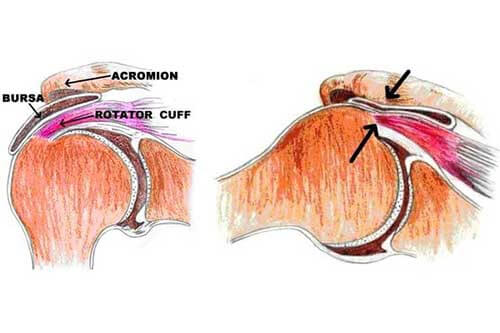
A combination of muscles and tendons keeps your arm bone centered in your shoulder socket. These tissues are called the rotator cuff. They cover the head of the upper arm bone (humerus) and attach it to your shoulder blade (scapula). The collar bone (clavicle) connects the shoulder complex to the rest of the body and the wing bone (scapula) rests on the rib cage. A portion of the wing bone (scapula) extends over the shoulder and acts as a roof over the humeral head. This is called the acromion and attaches to the end of the collar bone (clavicle) at the acromioclavicular joint.
Another portion of the scapula which sticks out is called the coracoid and this bone acts as the attachment point for 2 very important ligaments which go up to the collar bone (the coracoclavicular ligaments) as well as several muscles which travel down the arm.
The rotator cuff is a group of 4 small internal muscles, Supraspinatus, Infraspinatus, Subscapularis and Teres Minor.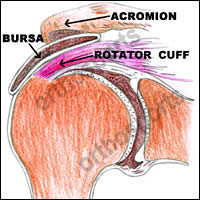
Over the top of the shoulder are larger muscles like the Deltoid, Pectoralis Major and Latissimus Dorsi. The small muscles work together to stabilise the glenohumeral joint and initiate the motion to allow the bigger muscles to help get your arm up over your head.
In order for the arm to be raised up in the air all of these complex parts must each play a role. Weakness or damage to any element will cause problems when trying to use the arm. This is why rotator cuff injuries usually result in weakness, especially when trying to raise the arm overhead. The muscle that is most commonly injured is called the supraspinatus muscle and this is the one found between the acromion bone (roof of the shoulder) and humeral head (ball of the shoulder) where it can get pinched and damaged.
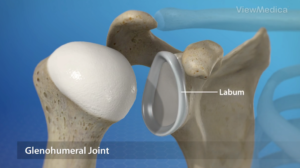
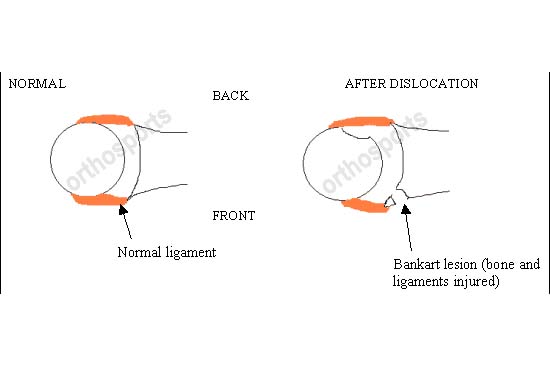
The humeral head (ball) is quite round and the glenoid (part of the scapula or wing bone) is flat. This leads to very good movement but should also allow the humeral head to fall off the glenoid (shoulder dislocation or separation). Luckily there is a structure called the labrum which runs around the edge of the glenoid and deepens the socket to aid in stability.
Our shoulders are used constantly in our day to day lives and while working. This includes pushing, pulling, lifting, and throwing. From the moment we wake up until we go to bed our shoulders are being used. Dressing, bathing, feeding, working, playing sport or just doing things for fun. The trade off for more mobility is the possibility of dislocating the shoulder or damaging the rotator cuff muscles which are helping to keep the shoulder in joint. Damage to the shoulder may result from repetitive movements, manual labor (particularly heavy overhead work), sports, aging or an accident or bad fall.
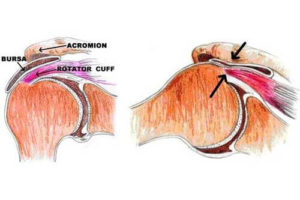
Across all age groups the most common cause of shoulder pain is impingement. Typically the Supraspinatus tendon is inflamed and pinches under the acromion (also known as bursitis). In the younger age groups this is closely followed by instability or dislocation of the shoulder. As you get older you are more likely to have a rotator cuff tear or frozen shoulder (often over diagnosed) and eventually this can lead to arthritis of the shoulder as you continue to age.
Fractures or broken bones tend to happen to younger people from sporting accidents or to older people as their bones get weaker with age. Much more rare are issues like infection, cancer or metabolic problems and impingement remains the most common diagnosis overall.
Of course it is possible that the pain you are feeling in your shoulder is coming from a problem in another part of your body, such as your neck (referred pain). Pain that travels past the elbow, is felt in the trapezius muscle (next to the neck), travels down the spine or into the wing bone or creates numbness or tingling in the fingers is almost always from the neck and not from the shoulder.
As a general rule, if you have had an injury or are experiencing a lot of pain it is best to see a doctor right away to have your shoulder condition diagnosed accurately. If you have general, mild shoulder pain which has developed slowly over time it is worthwhile adjusting your activities, taking nonsteroidal anti-inflammatory drugs (if it safe to do so), and learning some exercises from a physiotherapist to see if the pain improves on its own. If the pain is still there 6 weeks later medical treatment should definitely be sought.