What is Arthritis?
The simplest definition of arthritis is: damage to the shiny white joint lining cartilage (articular cartilage) in the shoulder (glenohumeral) joint.
While the small acromioclavicular joint can get arthritis it is a different type of joint which rarely needs surgery.
The glenohumeral joint is a ball-and-socket joint lined with articular cartilage which can wear out like a knee or hip joint does. The shoulder is not a load bearing joint and therefore does not wear out as often as the hip and knee do. As the articular cartilage in the shoulder breaks down the joint becomes rough and start to grind. As with other joint in the body the lining capsule becomes thickened and the joint loses motion as it gets stiffer. While there are many other types of arthritis such as: rheumatoid, psoriatic, infective, avascular necrosis and post-traumatic; osteoarthritis remains by far the most common.
The symptoms of shoulder arthritis are cyclical and can vary from day to day. They typically slowly get worse over time until eventually they become intolerable.
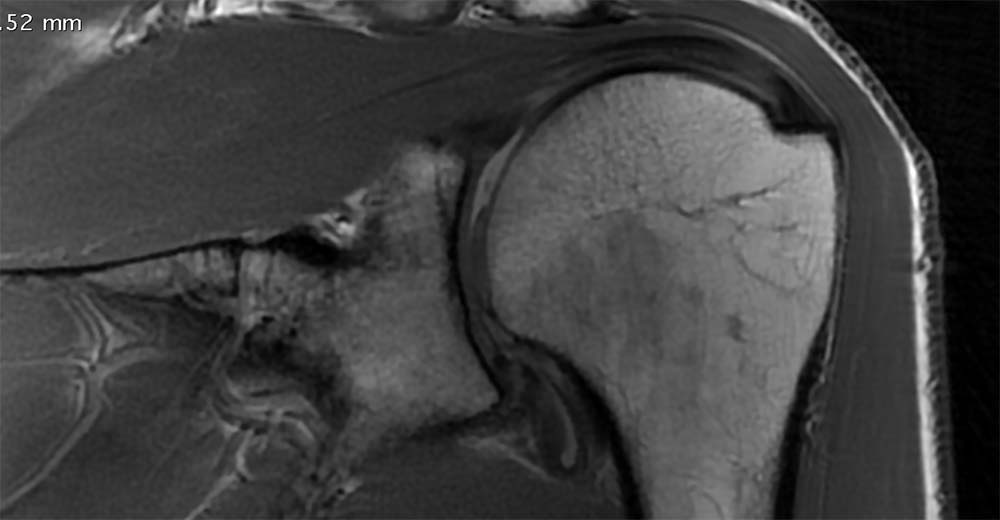
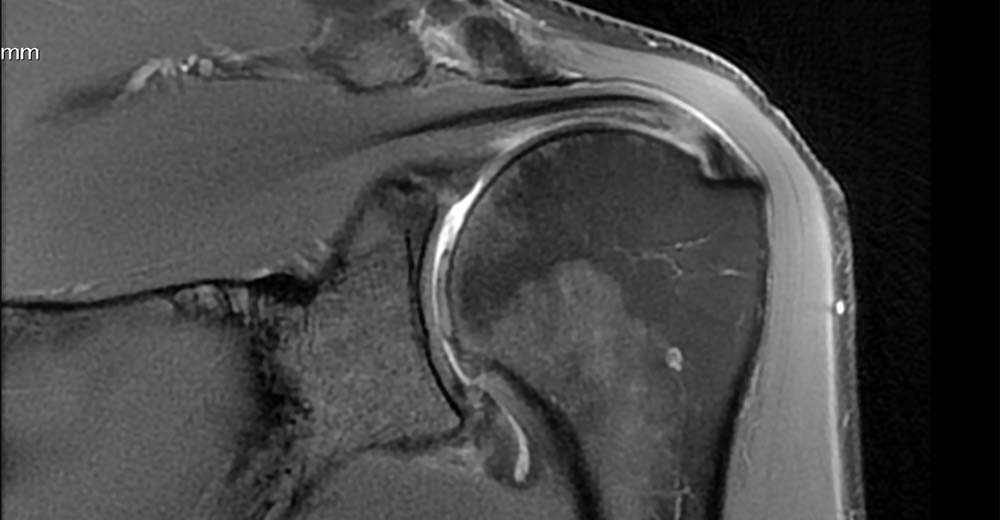
Diagnosis
The diagnosis of shoulder arthritis is made on a simple plain x ray where the joint space is narrowed and sometimes an osteophyte (overgrowth of bone called a ‘beard’ osteophyte because it is on the head of the humerus) will be seen. Some people have relatively normal looking x rays and the diagnosis is made on MRI scanning.
Pain Management
Many people learn to tolerate the arthritis and adapt their lifestyle to cope with the loss of motion. NSAIDS (anti-inflammatory tablets) can be used to control the pain but physiotherapy typically makes the pain worse and is best avoided.
Typically the patient describes pain in the front, side or back of the shoulder. The pain can be there at rest and is usually worse at night time. Lifting, carrying and exercising are extremely difficult and there may be grinding, clicking or cracking (crepitus) in the joint.
Many patients with shoulder arthritis are elderly and are unable to take anti-inflammatory medications. Ice packs are a very safe and effective option to reduce the pain and can be used several times a day if needed. 20-30 minutes of ice on the shoulder just before bed can improve sleep quality in some people.
In the early stages of arthritis cortisone injections can be useful to help control the pain and improve sleep. As the disease progresses the injection become less and less effective.
Surgery for shoulder arthritis depends on the age of the patient, the quality of their rotator cuff and the degree of bone damage or changes present.




Arthritis is far less common in the shoulder than it is in weight bearing joints like the hip and knee. There are many forms of arthritis with osteoarthritis being the most common form. If the joint lining wears out the joint will become painful and stiff and a shoulder replacement will be the only option to relieve the pain.
Most patients are in hospital for 2 to 3 days to learn how to shower and dress themselves while using a sling. There is no in-hospital physiotherapy for the shoulder.
The rotator cuff is very important to move the new shoulder. Typically patients wear a sling for six weeks after the surgery before starting physiotherapy. This allows the rotator cuff to heal. If the rotator cuff does not heal the new shoulder joint can dislocate. At 6 weeks active range of motion exercises start and at 3 months a gentle strength programme commences. It typically takes 6 months to recover properly from the surgery.
The joint replacement is made of a various metals combined together which are relatively inert and well tolerated by the body. Metal is placed in the humerus as well as being attached to the glenoid bone. Between them is a high grade medical plastic called polyethylene which allows friction free movement between the components. This can wear out after many years so you will need to have regular xrays performed to ensure that the prosthesis continues to function well. Changing the plastic liner is a relatively easy procedure with little down time but with the modern technology is rarely necessary.
Since the metal and plastic components are quite small they can be ‘rocked’ out of the bone with excessive lifting. It is recommended that you lift less than 2kg on a regular basis with an occasional 5kg lift being acceptable. If you have a pyrocarbon hemi-arthroplasty you are probably OK to lift whatever you are comfortable doing.
The answer to this question is not really known. In the past we did not recommend that people play golf just in case they caused loosening of the implants in the bone. A large number of people have ignored this advice and seem to be OK but we do not know if there will be any long term consequences of doing so as it has not been carefully studied.